

Education in the other SDGs: a gender perspective in health, water, sanitation and agriculture
Education in the other SDGs: a gender perspective in health, water, sanitation and agriculture
Education is key to achieving the SDGs, because education and training help develop professional capacities in each and every sector and because education influences the achievement of other development outcomes.
Education helps develop men and women’s capacities to implement development strategies…
Every sector needs enough qualified professionals to ensure service delivery and all sector human resource strategies need to focus on gender mainstreaming so that men and women can be equal participants in the workforce. More attention must be paid to the institutional barriers faced by female workers in the health, water and sanitation, and agriculture sectors, as well as to gender stereotypes across professions.
…IN THE HEALTH SECTOR
Women are pivotal in the health care workforce (Langer et al., 2015). Nurses, community health carers and home carers are primarily female. One estimate has suggested that, in many countries, women make up over 75% of the health workforce (WHO, 2008). SDG target 3.c aims to increase health financing and improve the recruitment, developing, training and retention of the health workforce in poorer countries. Using a minimum threshold of 4.45 doctors, nurses and midwives per 1,000 people, the World Health Organization (WHO) estimated that there was a global shortage of 17.4 million healthcare workers in 2013, which included a shortage of 2.6 million doctors and 9 million nurses and midwives (WHO, 2016). Countries with the heaviest disease burden are also those with the lowest density of health professionals, and the same applies within countries, with rural areas lagging behind urban ones (Crisp and Chen, 2014).
With regard to nursing, the most recent global strategic vision prioritizes education and recruitment, improved involvement in health policy development, collaborative partnerships, and increased political will to invest in effective evidence-based nursing and midwifery (WHO, 2016). The shortage of faculty to teach in schools of nursing is also an issue; lack of adequate incentives in academic programmes, reduced full-time equivalent positions and the global migration of nurses are factors in reducing the availability of trained staff to provide nursing instruction (Nardi and Gyurko, 2013). A 2010 study of Kenyan training institutions showed gender inequities that need to be addressed. Men and women were concentrated in different cadres; for example, pharmacy was considered a male job. Although the nursing profession is feminized, 80% of professors in nursing-only institutions were male (Newman, 2014).
In some countries, attempts have been made to recruit more male nurses. A key barrier to male nurse recruitment is the need to fight the stereotype that nursing is a female profession. In the United States, institutions have been set up to combat stereotypes around the nursing profession. For instance, the American Assembly for Men in Nursing encourages men to enrol in nursing programmes, with a goal of increasing male enrolment to 20% by 2020 (AAMN, 2018; MacWilliams et al., 2013).
Trained community health workers play an important role in alleviating staff shortages (UNESCO, 2016a). Community health workers are typically local residents with basic education who receive vocational training. Remuneration strategies vary, ranging from volunteers to fully paid positions (Olaniran et al., 2017). Community health workers have substantially contributed to reducing maternal and child mortality around the world. In the United States, they are also helping to reduce the disease burden from non-communicable diseases, such as hypertension and cardiovascular problems, especially for hard-to-reach populations (Perry et al., 2014). With respect to acceptance by the community, analysis from the United Republic of Tanzania found that men were more likely to be comfortable with male workers and women with female workers in discussing health issues (Feldhaus et al., 2015).
In Brazil, Ethiopia, India and Pakistan, community health worker programmes have been substantially scaled up, and countries have made efforts to integrate community workers into health systems (Zulu et al., 2014). For instance, under the Brazilian Special Service for Public Health programme, 240,000 health workers provide home visits to 110 million people. In Pakistan, the Lady Health Worker Programme has over 90,000 workers serving 70% of the rural population. India has one of the largest systems, including 800,000 accredited social health activists, 1.2 million anganwadi (or local mother-and-child health) workers and over 200,000 ancillary nurse midwives (Perry et al., 2014). In recognition of the importance of this type of programme, in 2017, 23 country delegations laid out plans to institutionalize community health systems, in collaboration with USAID, UNICEF, WHO and the Bill and Melinda Gates Foundation (Zambruni et al., 2017).
Several challenges need to be addressed to improve working conditions for health workers. Women in nursing, community health work and home care have been found to privately make adjustments for systemic challenges they face in their profession, furthering gender inequalities in the healthcare system and society (George, 2008). Female community health workers remain under-recognized, underpaid, overworked and under-supported (Zambruni et al., 2017). Community health workers also often suffer from gender-based violence, and stronger efforts must be made to provide them with a safe working environment (HIFA, 2017).
…IN THE WATER AND SANITATION SECTOR
More female involvement is needed if target 6.b, improving local communities’ participation in improving water and sanitation management, is to be achieved. Women are the frontline workers in the sector as communitybased sanitation workers, yet, in some contexts, men are the primary decision-makers in terms of investment and construction of latrines. There is a significant shortage of qualified professionals in the sanitation sector. The 2012 Global Analysis and Assessment of Sanitation and Drinking-Water (GLAAS) report from 74 developing countries showed that women made up less than 10% of the professional workforce in half the surveyed countries (WHO and UN Water, 2012).
An analysis of 12 low and middle income countries found that female professionals constituted 17% of the workforce, on average, ranging from a low of 7% in Papua New Guinea to a high of 35% in Burkina Faso and South Africa (International Water Association, 2014). Policies to improve the gender balance in water utilities need to include improvements in education, investment in networks and increased use of legal tools (Das and Hatzfeldt, 2017). In Peru, the government enacted a law of equal opportunities in 2007 to address governance and gender relations. Local governments adopted this law and small town water suppliers introduced reforms to ensure men and women have equal representation in water management oversight boards. In the United Republic of Tanzania, the National Water Policy required local community water committees to ensure equal representation of men and women and to implement a meritbased gender-sensitive recruitment policy. In Uganda, reforms undertaken after an institutional review in 2003 increased female representation in management positions at the Ministry of Water and Environment from 0% to 18% (Water and Sanitation Program, 2010).
In South Africa, the national gender policy recommends that rural women should be trained in pump and water systems management and repair. A Working for Water project created 180,000 full-time jobs over the past two decades and ensured that 52% of the benefits from training and income generation accrue to women by requiring that resources are allocated in a gender-aware manner (International Water Association, 2016).
… AND IN THE AGRICULTURAL SECTOR
Agricultural labour is often misconstrued as a male domain, despite the fact that women constitute about half of the sector worldwide. In richer countries, there has been a resurgence of female farmers and a growing interest among women in agricultural higher education. In the United Kingdom, the number of women running farms increased by nearly 10% between 2010 and 2013 and 28% of the agricultural workforce is female. Agriculture related courses at universities and colleges attracted 25% more women than men in 2015 (UK DEFRA, 2016). In Australia, since 2003, female enrolment in agricultural universities has exceeded male enrolment, with agriculture now considered equally appropriate for both genders (Pratley, 2017).
Women make up less than half of agricultural researchers employed in government, academia and non-profit organizations but there are enormous variations among countries (Figure 10).
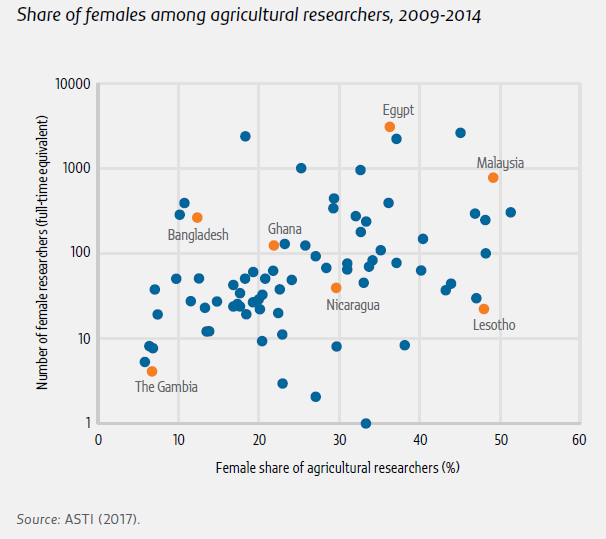
In sub-Saharan Africa, across 39 countries, approximately 27% of researchers were female. As in many other sectors, women’s participation declines in higher level positions and women face many challenges prior to and during their scientific careers (Beintema, 2014).
Education has important interactions with health, water and sanitation, and agriculture
Education is both shaping and being shaped by development challenges. This section discusses examples of relations between education and outcomes in three sectors.
Education influences preventive behaviour against non-communicable diseases
In 2012, non-communicable diseases including cancer, diabetes, chronic respiratory and cardiovascular diseases, along with those caused by alcohol, tobacco, excessive sodium and insufficient physical activity, accounted for 68% of deaths worldwide, three-quarters of which occurred in low and middle income countries (WHO, 2014). The mediating influence of education on non-communicable diseases operates through different channels. Education affects behaviour through cognitive and psychological processes, wealth and status, and empowerment. Initially, education may negatively affect health behaviour, as a better-educated population can afford unhealthy lifestyles. As availability of accurate health information increases, the relationship between education and healthy behaviour becomes positive, although there can be variations by gender (Baker et al., 2017).
Formal and non-formal education can help reduce obesity
Obesity worldwide more than doubled between 1980 and 2014. The epidemic is increasingly global, and no country has experienced substantial declines over the last three decades. Among adults, obesity was more than 50% among women in countries in Northern Africa and Western Asia (Kuwait, Libya and Qatar) and the Pacific (Kiribati, the Federated States of Micronesia, Samoa and Tonga) (Ng et al., 2014). A systematic analysis of 91 countries showed that the relationship between educational attainment and obesity varied by country income and overall prevalence (Cohen et al., 2013). In low income countries with a low prevalence of obesity (with a few exceptions, such as Cambodia), the most educated women were the likeliest to be obese. In middle income countries with a higher prevalence of obesity, such as Colombia, the Dominican Republic and Peru, the opposite was true (Figure 11).

In high income countries, tertiary education is linked to a lower probability of obesity among both women and men. In 24 OECD countries, 19% of adults were obese in 2011, and adults with a tertiary education were half as likely to be obese as those with less than upper secondary education. Of those with less than upper secondary education, 28% of women (and 22% of men) were obese, compared to 12% of women (and 15% of men) with tertiary education (OECD, 2013). This finding was supported by an analysis of longitudinal data on identical male twins in Australia, which found that education also reduced the probability of being overweight (Webbink et al., 2010).
Being obese or overweight is more and more linked to education and socioeconomic inequality. A comparison of 34 countries in North America and Europe in 2002, 2006 and 2010 found that socioeconomic inequalities in health were increasing, as measured by levels of physical activity and body mass (Elgar et al., 2015). In OECD countries, obesity has been rising rapidly among less educated men and among average educated women, except in the United States. For instance, in the Republic of Korea, less educated women were five times more likely in 2010 to be overweight or obese than those with higher education, whereas in 2014, they were six times more likely (OECD, 2017a).
Physical activity is an important healthy behaviour that may help reduce obesity. In 2010, more than 80% of school-going adolescents aged 11 to 17 years were not sufficiently active, that is, participating in at least 60 minutes of moderate to vigorous physical activity per day. In most countries, girls were less physically active than boys (WHO, 2014).
In some instances, adolescent girls’ physical activity and movement are restricted by legal and cultural norms. In Saudi Arabia, obesity is a general public health concern but a worse issue among girls than boys, with at least some of this challenge linked to restrictions on physical activity and education for women and girls (Mahfouz et al., 2011). In Philadelphia, United States, adolescent girls were far less likely to be active than boys – 28% of girls were sedentary compared to 11% of boys (Lenhart et al., 2012).
A review of school-based physical activity programmes across 44 studies found that printed educational materials and changes in school curricula to promote physical activity had positive health outcomes and succeeded in increasing the duration of physical activity among students (Dobbins et al., 2013). Non-formal and informal campaigns also make a difference. In Tonga, the national strategy to prevent and control noncommunicable diseases was used to promote physical activity among women and encourage them to play netball. Since 2012, it has delivered community mobilization updates, advertising campaigns and interpersonal education (WHO, 2014).
Education is linked to lower tobacco use
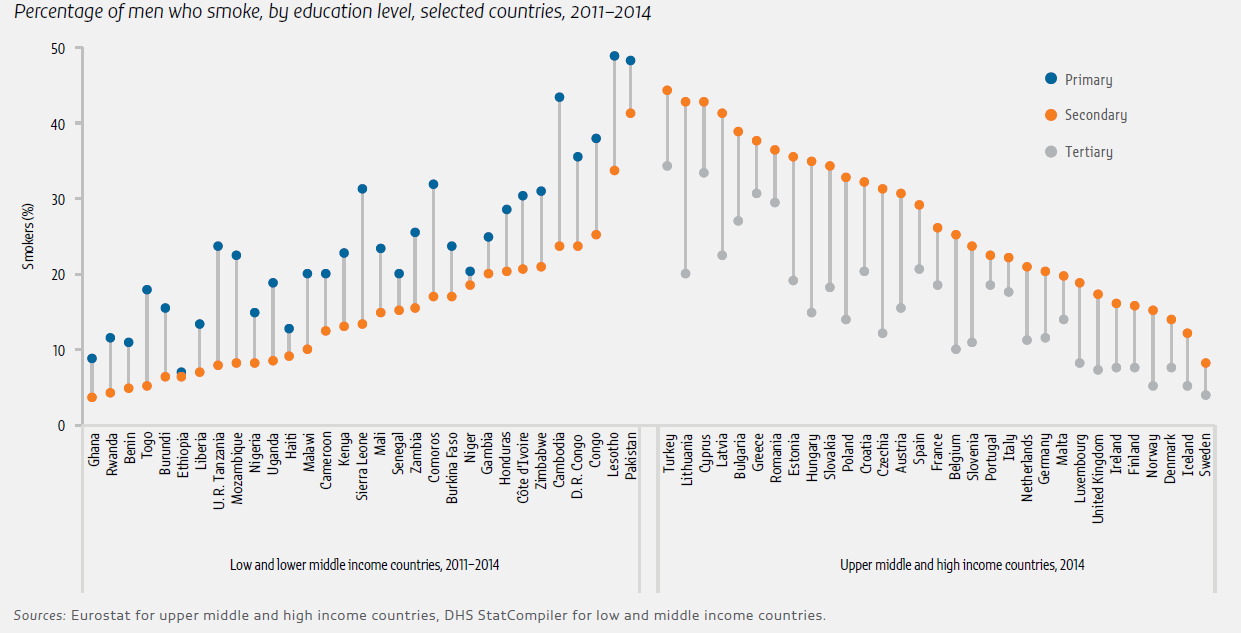
Tobacco is a leading cause of preventable deaths worldwide; 6.4 million people died as a result of tobacco use in 2015. Globally, in 2012, 21% of adults smoke: 36% of men and 7% of women. In the OECD, 23 countries had data on smoking, showing that 44% of men and 32% of women with less than upper secondary education smoked, compared with 24% of men and 19% of women with tertiary education. The impact remains strong even after controlling for age and income effects (OECD, 2013). Disaggregating tobacco use by education level shows that in poor and rich countries alike, men with more education are less likely to use tobacco (Figure 12).
Smoking prevalence globally has increased among women with a lag, as cultural norms change. While tobacco consumption correlates negatively with education, this relationship has increased over age cohorts and is different for men and women. In France, in the oldest cohort, less educated men were 1.5 times as likely to smoke as the most educated; in the youngest cohort, less educated men were 5 times as likely to smoke as the most educated. Among women, the oldest cohort of more educated women were twice as likely to smoke as less educated women; in the youngest cohort, less educated women were 3.7 times as likely to smoke as more educated women (Pampel et al., 2015).
Tobacco companies have turned their attention to poorer countries around the world, where consumption continues to increase. Data from global tobacco surveys show that the number of female adolescents who smoke tobacco in African countries vastly exceeds the number of adult women, due to increased marketing and tobacco access. For instance, in the Gambia, 3% of adult women but 37% of adolescent females were found to be using some tobacco product (Good Business, 2016). A gender-sensitive global response to control tobacco use is needed. However, most national guidelines for treating tobacco dependence are gender neutral or gender-blind (Bottorff et al., 2014).
The tobacco industry has systematically marketed cigarettes with a gender-differentiated focus, using feminine or masculine qualities in their campaigns to appeal to different target demographics. For instance, historically, the advertising industry spent billions to attract women by suggesting that smoking would make them thinner (Amos and Haglund, 2000; Cole and Fiore, 2014; Marine Street, 2012). In Indonesia, a country with some of the highest male smoking rates, tobacco advertising is highly prevalent, and smoking is strongly associated with masculine identity (Ng et al., 2006; Nichter et al., 2009). Informal education can affect smoking habits. Hard-hitting health warnings are among the most effective deterrents. Between January 2009 and June 2014, the number of countries running comprehensive national mass media anti-smoking campaigns lasting at least three weeks increased from 23 to 39 (WHO, 2015b).
Educating young people about advertisements that target them can best be achieved by using the same marketing methods that have been successfully employed by the tobacco industry (Barbeau et al., 2004). In some countries, father and family-man images have been used to challenge the association between smoking and masculinity in order to encourage men to quit smoking (Bottorff et al., 2014). In Botswana, a social media based intervention encouraged girls to use specific phrases to note their decision not to smoke. The campaign has become embedded in teenager social life and is also highly popular on Facebook (Good Business, 2016).
WATER AND SANITATION ISSUES NEGATIVELY AFFECT GIRLS AND WOMEN
Water and sanitation quality has major effects on child cognitive development and brain function, influencing lifelong learning capacity (Piper et al., 2017). But there are also other links between water, sanitation and education.
Girls and women are most often responsible for hauling water, especially in rural areas. As a result, lack of easy access to water for household usage has a detrimental effect on school attendance (UNESCO, 2015a). In Ghana, an analysis of four rounds of data from the Demographic and Health Surveys between 1993 and 2008 found that reducing the time to fetch water by half increased girls’ school attendance by about 7 percentage points (Nauges, 2017). An analysis of 24 sub-Saharan African countries estimated that 13.5 million women and 3.4 million children spend more than 30 minutes each day collecting water for household use; in all countries, girls were more likely than boys to have the responsibility of fetching water (Graham et al., 2016).
Climate change and population growth increase water insecurity and intensify the impact on education. For instance, in Botswana, more than half of girls spent more time fetching water for domestic use during droughts (Chigwanda, 2016). In Gujarat and Rajasthan states, India, a survey of secondary school students from 500 families who attended 8 secondary schools revealed that more than 90% viewed groundwater scarcity as a major issue affecting their education. On average, 60% of the students missed about two days of school a month. In Rajasthan, female students missed at least five days of school a month at rates two to ten times as high as male students (Kookana et al., 2016).
Policies focused on increasing access to water-related infrastructure are important in reducing the time spent on these chores. In Nepal, a community-based water supply and sanitation project targeted access to latrines, to provide a safer environment for women and reduce the time it takes to manage household water supply. The average time for fetching water was reduced from 3.8 to 2 hours per day, which freed up time for education activities (Asian Development Bank, 2015). In China, a major water treatment programme, which started in the 1980s, benefited rural girls to the extent that the education gender gap in treated villages was eliminated (Zhang and Xu, 2016).
Slums also face water shortages. In low-income housing areas in Blantyre, Malawi, populations in peri-urban areas lack access to portable and safe water. In unplanned areas, girls often stay away from school to help their mothers collect water (Chipeta, 2009). In Delhi, India, 20% of residents live in slums and settlements. Mothers reported that girls missed school for different chores, including water collection, a situation that had worsened because of growing slum populations, increased droughts and unpredictable rainfall (Kher et al., 2015).
Menstrual hygiene management is a key issue in schooling for adolescent girls
Menstrual hygiene is a public health issue that requires better planning (Mahon and Fernandes, 2010). The global visibility of the issue has increased in recent years (Sommer and Sahin, 2013). However, consistent financing policy measures on sanitation were targeted at women in only 11 of 74 countries surveyed (WHO and UN Water, 2017).
The lack of adequate sanitary care for adolescent girls has several consequences for education. In Bangladesh, a nationally representative study from 2013 found that 41% of schoolgirls aged 11 to 17 in Bangladesh reported missing 2.8 days of school per menstrual cycle (Alam et al., 2017).
A recent analysis of policy documentation in schools in 21 low and middle income countries found little focus on menstrual hygiene management in education sector plans (Sommer et al., 2017). A study in rural areas of Ethiopia, Kenya, Mozambique, Rwanda, Uganda and Zambia found that less than 20% of schools had at least four out of the five recommended menstrual hygiene services (separate sex latrines with doors and locks, water for use, waste bins) (Morgan et al., 2017).
A feasibility study in rural Kenya examined water and sanitation facilities in 62 primary schools during unannounced visits. It found that 60% had water for handwashing, 13% had washing water in latrines and only 2% had soap (Alexander et al., 2014). Data on water, sanitation and hygiene expenditures in 89 rural Kenyan primary schools showed that expenditures averaged US$1.83 per student per year, while the estimated cost to meet basic standards was US$3.03 per student per year (Alexander et al., 2016).
Policy awareness of the issue is increasing in some countries. In India, the government in 2010 proposed a new scheme to provide subsidized sanitary napkins in rural areas (Garg et al., 2012). Analysis from 28 states and 4 union territories in India between 2007 and 2015 found that providing separate female toilets in schools is positively associated with enrolment and participation at the upper primary level. However, this does not improve the situation for scheduled caste populations, which hints at further equity challenges linked to untouchability (Ray and Datta, 2017).
Other challenges include fighting negative attitudes towards menstruation and increasing the provision of health information and facilities in schools (Sommer et al., 2015). In rural Bolivia, girls received limited information on menstrual hygiene management from teachers and parents, which suggests the need for its inclusion in school curriculum and national policies (Johnson et al., 2016).
EDUCATION INTERVENTIONS ARE NEEDED TO REACH OUT TO FEMALE FARMERS
Improving agricultural productivity is a key target in SDG 3. In 2010, women made up around 50% of the agricultural labour force in sub-Saharan Africa. Women’s productivity per hectare is estimated to be lower than men’s, which is mostly due to limited access to land, technology and other inputs. If women had the same access to resources, then their yields would increase by 20% to 30% (FAO, 2011).
Men have higher input measures than women, in terms of inorganic fertilizer, seed varieties and extension services (Peterman et al., 2014). In northern Nigeria, women produced 28% less than men. However, after controlling for observed factors of production, there were no differences in the south of the country (Oseni et al., 2015). A productivity differential between men and women was also observed in Ethiopia (Aguilar et al., 2015). In Uganda, men were found to use more inputs, and the main difference between men and women was linked to childcare responsibilities (Ali et al., 2016).
The gap in productivity suggests a need for improved training and support. It has long been understood that agricultural extension and advisory services often do not reach women. An analysis of access to extension services in Ethiopia in 2010 found that female heads of households are less likely to have access to extension services (Ragasa et al., 2013). An earlier analysis in Nigeria found that women farmers who were supervised by female extension agents were more likely to have more access to extension services and to show higher levels of awareness and participation, which suggests that extension organizations should recruit more female extension agents (Lahai et al., 1999). An analysis of the quality of the advice received by women in Sri Lanka found that women had more discussions on their crops with female ‘plant doctors’ (Lamontagne-Godwin et al., 2017).
However, it has also been suggested that in order to move towards gender-equitable control over assets and resources, the focus should be on collaboration between men and women rather than just on targeting women (Russell et al., 2015). In the eastern Democratic Republic of Congo, joint male and female programme participation in agricultural extension programmes was found to lead to the highest adoption of technologies such as improved legume varieties, row planting and mineral fertilizers, more so than efforts targeting just female farmers (Lambrecht et al., 2014).
Other research suggests that gender-specific responsibilities, resources and constraints need to be factored in by agricultural development programmes if they are to benefit men and women shareholder farmers. Coming up with sex-disaggregated measures for agricultural productivity is riddled with assumptions, which means that the conventional wisdom that productivity is lower for women is difficult to fully confirm. But since women perform a larger share of other household tasks, some argue that the answer to enhancing women’s agricultural productivity lies beyond the agricultural sector, in interventions that can alleviate women’s drudgery – such as through improving access to water and improving child health and education (Doss, 2017).